
History: 3 day old boy, presented to CSC with his mother with a congenital deformity of the left foot. The baby was born at full term, first child in the family with no other family history of congenital foot defects. The mother does not feel there are any other abnormalities with the child.
Dr Saqib: Learning point 1: Remember not every congenital foot deformity is club foot! There are different foot deformities at birth and you should know about them all and be able to recognise: metatarsus adductus, club foot, calcaneovalgus, congenital vertical talus, amniotic band, syndactyly, polydactyly. Read this article for more information about all these conditions:
The Newborn Foot Remember any congenital abnormality can be associated with other problems for the baby, including abnormalities in the face, spine, hips, knees or internal organs.
Dr Saqib: Learning point 2: Any newborn or child who presents to CSC must have full examination, including looking for facial abnormalities, spine, upper limb, hips, knees and feet. All the findings, even if normal, must be written in the electronic notes. For example: Normal face, normal spine, normal hips, normal knees.
It is also important to screen the hips for dislocation.
Dr Saqib: Learning point 3: With every new born baby you examine, you can screen for hip problems by performing the Barlow and Ortolani test. You can review the video here:
Barlow and Ortolani test on YouTube. Calcaneovalgus presents with the ankle is severe dorsiflexion and hindfoot eversion. It can be associated with postero-medial tibial bowing, DDH and torticollis. However, when the foot is in this position, you must also consider congenital vertical talus.
Dr Saqib: Learning point 4: A big difference between calcaneovalgus and congenital vertical talus is whether the deformity is rigid or flexible. Therefore it is important to examine the flexibility of the foot and write this in the notes. Look at the examination below. Calcaneovalgus is usually flexible, vertical talus is rigid.
The child presenting to CSC had a flexible foot.

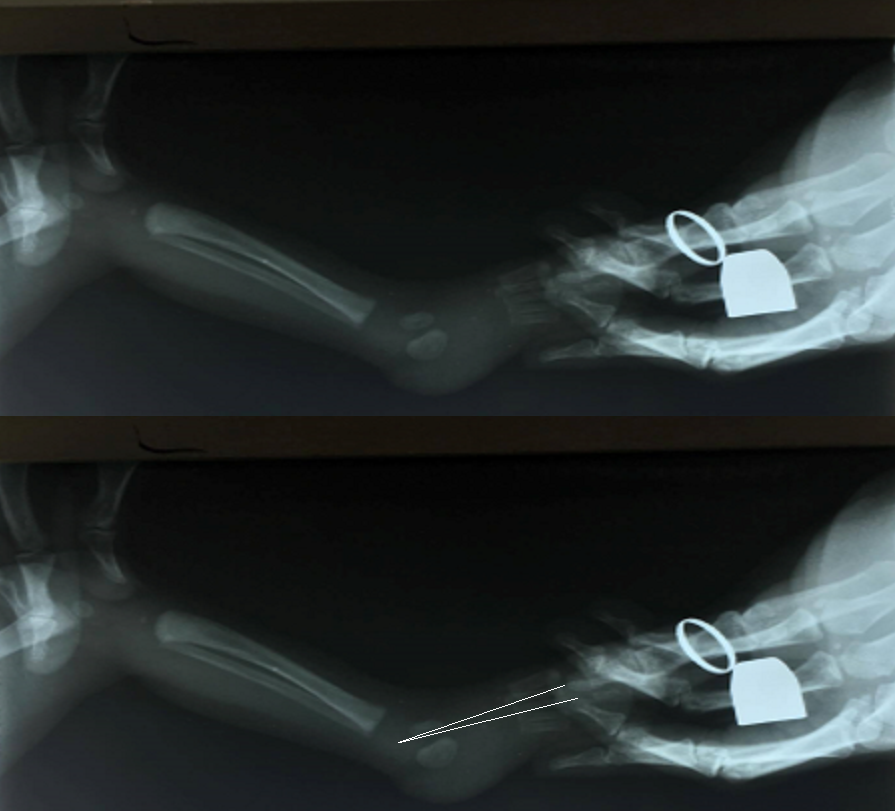
Another way to help differentiate between calcaneovalgus and congenital vertical talus is an x-ray.
Dr Saqib: Learning point 5: With a lateral x-ray, you can review the angle of the talus and the first metatarsal (the navicular bone does not show on x-ray til around age 3). You can assess Meary’s angle to look for vertical talus. Look at our x-ray below. The angle between the talus and the first metatarsal is small, and therefore we do not have congenital vertical talus in our patient.
You can read more about Meary’s angle and congenital vertical talus here and an example of congenital vertical talus x-ray here.
The treatment for calcaneovalgus is stretching excercises and sometimes a cast if it is not improving. Read more about calcaneovalgus foot and treatment here.
If you want to read about the management of congenital vertical talus, read the article below – A new approach to the treatment of congenital vertical talus – Farhang Alaee Æ Stephanie Boehm
[gview file=”http://teaching.csc.org/wp-content/uploads/2017/09/s11832-007-0037-1.pdf”]